


Kansas COVID Weekly, 11Feb2021
Kansas COVID-19 Updates

Vaccine Update
Kansas is ranked #31 in the nation in terms of vaccine doses distributed to the state per 100,000 by the federal government (last week #25), and #49 of states in terms of persons receiving at least 1 dose per 100,000 residents (last week #47). According to NPR, 6.6% of the Kansas population has received at least one dose of the vaccine. The state has used 58% of its dose allocation, ranking it #50 in the nation. What does all of this mean? It means that Kansas is failing at the vaccination effort. The state needs to be doing more to organize and administer the vaccines it has available. It’s really, really not okay. Those doses represent lives saved (or not saved), which is even more urgent this week as we record our deadliest week (by date of report) in the pandemic since it began.
You can see the Kansas vaccine information page here. The Centers for Disease Control and Prevention COVID-19 Vaccine Data Tracker is also a useful too, but be advised that the Kansas numbers are only updated with them on Monday, Wednesday and Friday.
The New York Times has a vaccine tracker now and they project that given the current pace of immunizations, the nation will reach 70% of the population partially vaccinated by early September. We can move this date sooner by improving our current pace. This depends on efficient use of existing supply (a state responsibility) and greater supply of vaccine (a federal responsibility).

I think that while this graph is daunting, it frames the vaccine effort in a new way - this is the race back to “normal.” So whereas Kansas has administered 2 doses to 2.6% of its population (#40 in the US), West Virginia (#1) has done so for 6.2% of its population. The states that win this race will have faster economic recovery as well as saving countless lives along the way. So we really should be throwing everything we have behind this effort. The deaths we’re experiencing are preventable, both through limiting community transmission and now a vaccine. By inefficiently using the vaccine doses available, the state is surrendering preventable deaths and its economic growth.
I’ve done some additional writing on the COVID vaccines recently.
Some early data on who is being vaccinated in the US, including demographic data for age, sex and race.
Vaccine safety data, including a discussion of the VAERS reporting system and its pitfalls.
The White House state report for Kansas can be viewed in full here. The summary table is provided below. Kansas is mostly in the red and yellow zones with good improvement over the past week. The exception is the death rate, which showed a big spike last week (+78%), a continuation of the previous week’s increase. Next week’s report will likely show a continuing increase in new death rate, given more recent trends.

Kansas has the following rankings within the US.
#22 for new case rate per 100,000 (red zone)
#30 for test positivity (yellow zone)
#30 for new hospital admissions per 100 beds for COVID-19 (orange zone)
#8 for new deaths per 100,000 (dark red zone).
Combined Data
The graph below shows us how some of our most important data points are moving over time. Cases are represented by the blue line and correspond with the left y-axis. All other metrics (hospitalizations, ICU admissions, deaths) correspond with the right y-axis.

Cases continue to drop, however the rate of decrease has slowed. Hospital admissions and ICU admissions have also declined. However, we’ve seen a big spike in deaths in the past week. It was the highest weekly death total to date. I should note that all of these data points are based on date of report. The state of Kansas shows metrics by date of occurrence, but it does not show us where newly reported cases/hospitalizations/deaths fit on that timeline as they are reported.
In other states, what’s we’ve seen is that when cases and hospitalizations surge, the deaths follow about 2-3 weeks later. But just as cases and hospitalizations decrease eventually, so too should deaths. Instead, what we’ve seen in Kansas is that following the surges in cases and hospital admissions, deaths have continued to escalate over time. This might be an artifact of delayed reporting. The evidence for this is offered when you look at the graph of deaths by date of death below. We aren’t seeing a big spike in recent history. But we don’t get to see where newly reported deaths are backdated as they’re reported. Whereas there’s typically a 14-day window of uncertainty for cases, death reporting can be even more delayed. It might be fair to expect a 30-day window of uncertainty for deaths. These large reports of deaths that don’t appear to be in the recent history would suggest that our death surge was even bigger than we previously realized. I asked the Kansas Department of Health and Environment for clarification on whether the record-setting number of deaths reported this week were the result of a data dump, a collection of delayed reports of deaths, all catching up at once. Their response was vague and didn’t really answer the question.

Another possible reason to suspect this “surge” in deaths might be due to delayed reporting is because we don’t see a surge happening in hospitalizations, a sign that there are more severe cases. Deaths don’t materialize out of nowhere. They have to get sick first and we aren’t seeing a surge in cases. They typically have a hospital stay prior to death and we aren’t seeing a spike in hospital or ICU admissions. The only thing I can point to if this *isn’t* a result of delayed reporting, is the possibility that we’ve had a number of people die in long-term care facilities, without a hospital stay. In fact, this week 92 new LTCF-associated cluster deaths were reported, about a quarter of the week’s death total.

Testing
The graph below shows us how Kansas is doing for tests performed (blue line, left y-axis) and the percent of those tests that are positive (red line, right y-axis) on a weekly basis. The goal line for test positivity (5%) is indicated by the gray, dashed line.
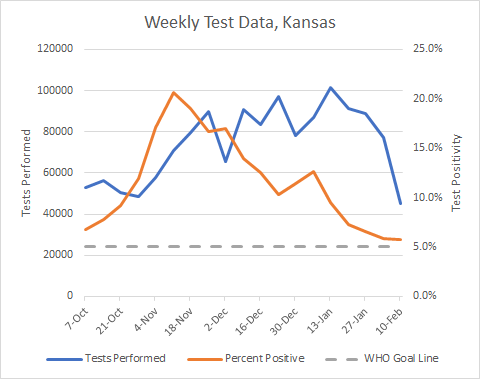
Test output has declined 51% in the past three weeks. So far, that hasn’t corresponded with an increase in test positivity - this can happen when you aren’t testing widely enough. And we’re nearly back to the goal line of 5% test positivity but have stopped the decrease and plateaued just above 5%. But I am really concerned about the decrease in testing output because while cases are declining the arrival of the more transmissible variant that has become dominant in the United Kingdom (known as the B.1.1.7 variant) has been found in several states (932 cases so far) and often these people don’t have a history of recent travel. That suggests that the variant has been spreading quietly throughout the country. The idea that Kansas has 0 reported cases so far does not mean it’s not here already. The US does not have a robust surveillance program to watch for this variant. We likely have many, many more of these cases than we realize. This variant is expected to result in a dramatic rise in cases. When I see the test output drop as it is here, then I worry that we will have a dramatic rise in cases (especially asymptomatic ones) that we can’t see or detect. It might make it harder for hospitals to see what’s coming. But we will see the impacts on hospital burden and death.
Cases
In the past week there have been 5979 cases newly reported by the Kansas Department of Health and Environment. That’s a decrease of 6.5% compared to the previous week. The weekly case rate per 100,000 residents for the state is only 3.2% above the pre-surge level, which is very good. We’ve almost come back to the pre-surge baseline. The case rate is lowest in Frontier counties and highest in rural counties. You can check to see your county’s classification here.

The map below comes from the Brown School of Public Health. It grades each county’s level of risk, based on the average daily cases per 100,000 over the most recent 7 days. Risk is greatest for red counties and least for green counties. Around the beginning of the year, the entire state was red. Now, we see definite signs of improvement, especially for the western half of the state.

Next, let’s look at where the most recent week’s cases are coming from in terms of age groups. The graph below shows 8 week timelines for each age group with the most recent week shown in maroon. One heads up, the “week” of 19-23Dec was a shorter week than usual so that week’s data are an anomaly.

It’s interesting to note that the decreases in cases have slowed and leveled off for many age groups. One age group (18-24) actually saw a small increase.
Hospitalizations
This week there were 262 newly reported hospital admissions compared to the week prior, a decrease of 17%. The graph below shows us where those hospital admissions are coming from in terms of age group, over the past 8 weeks. I want to again remind you to not worry too much about the week of 19-23Dec because it was a short week.

Many age groups saw a decrease this week with some decreases bigger than others. But an increase was noted for those 35 - 44.
There were 68 new ICU admissions in the past week for COVID-19, a decrease of 8.1% compared to the previous week.
Deaths
Using the HHS Community Profile Report (date 10Feb2021), Kansas has the 3rd highest newly reported death rate per 100,000 residents in the country, a big increase from where we were last week (21st).
In the most recent week, Kansas has reported a net increase of 408 deaths, an increase of 131% compared to the previous week. They more than doubled. The graph below shows us how deaths have trended over time, adjusted for each county type’s population size. The statewide average is shown in the black line. You can check your county’s classification here.

The death rate for Kansas has risen a lot but the previous weeks showed a really large drop. This further makes me believe that we have some delayed reporting going on and that they got caught up in the most recent week. The death rate spike we’re seeing now is largely driven by semi-urban counties (this county class includes Butler, Crawford, Franklin, Geary, Harvey, Reno, Riley, Saline). The bulk of the semi-urban deaths came from Butler, Crawford and Harvey counties.
We can also see where deaths are coming from in terms of age group in the graph below. Like the other demographic graphs, this shows 8-week timelines for each age group. This week we saw increases for all age groups except those 35-44. In fact, Kansas reported it’s first pediatric death last week, a 6 year old. The state does not provide any other data such as sex, race or county of residence for the pediatric death. My deepest condolences go to their family and community.

That’s it for now. See you next week!
References
https://covid.cdc.gov/covid-data-tracker/#vaccinations
https://www.kansasvaccine.gov/
http://www.ipsr.ku.edu/ksdata/ksah/population/popden2.pdf
WHCTF report repository: https://beta.healthdata.gov/Community/COVID-19-State-Profile-Report-Kansas/scin-7ddt
https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
https://beta.healthdata.gov/National/COVID-19-Community-Profile-Report/gqxm-d9w9
Kansas COVID-19 Updates is a free newsletter that depends on reader support. If you wish to subscribe please click the link below. There are free and paid options available.
My Ph.D. is in Medical Microbiology and Immunology. I've worked at places like Creighton University, the Centers for Disease Control & Prevention and Mercer University School of Medicine. All thoughts are my professional opinion and should not be considered medical advice.